Ectopic Pregnancy
Share this:




By Cesar Fortuna, M.D. Candidate, Class of 2022
What is an Ectopic Pregnancy?
An ectopic pregnancy is a pregnancy in which a fertilized egg during pregnancy has implanted outside of the normal location within the womb or uterus. Women suffering from an ectopic pregnancy can present in a variety of ways, most commonly in the 1st 3 months of pregnancy with lower abdominal pain and vaginal bleeding. These symptoms typically present anywhere from 6-8 weeks after the patients last menstrual period but can also present later.
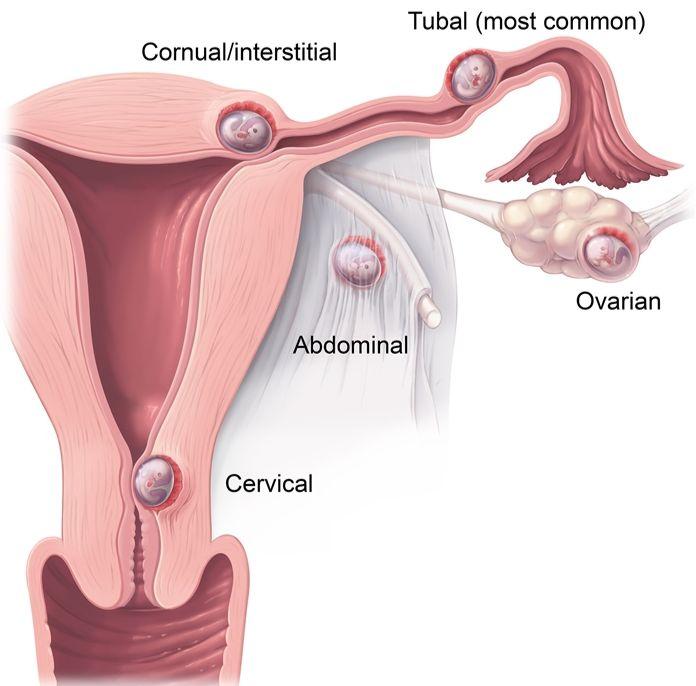
What are the different kinds of ectopic pregnancy?
Below are some of the different locations that can be involved in an ectopic pregnancy, with attachment to the fallopian tube occurring in 96% of cases; nonetheless all of them are abnormal. An untreated ectopic pregnancy can be a medical emergency.
What are the risk factors?
While all woman who are sexually potentially have a minor risk for an ectopic pregnancy, some women may be at much higher risk:
High Risk:
- previous history of an ectopic pregnancy
- previous pelvic surgery, abdominal surgery, or multiple abortions
- having structural abnormalities in the fallopian tubes that make it hard for the egg to travel
- current or past use of an IUD or use of Levonorgestrel IUD
- In Vitro fertilization in current pregnancy.
Moderate Risk:
- Being 35 years or older
- Current use of Estrogen or Progestin oral contraceptives
- Previous sexually transmitted infection (chlamydia or gonorrhea)
- Previous pelvic inflammatory disease
- Current or previous smoker
- Previous unexpected abortion
Low Risk:
- history of infertility
- previous medically induced abortion
- Age > 40 years+
- Use of vaginal douche
- Previous surgical removal of appendix
It is important to remember that even if you have one or a couple of these risk factors above, it doesn’t necessarily mean that you have or will get an ectopic pregnancy, but if you have symptoms you should speak with your gynecologist. Below is a list of these risk factors with an Odds Ratio, which is a statistical term to express how likely an ectopic pregnancy may be. When you meet with your gynecologist they will go over this information with you.

When do Gynecologists consider Ectopic Pregnancy as a diagnosis?
Ectopic pregnancies are considered by providers in any sexually active woman with vaginal bleeding or abdominal pain and:
-Are pregnant but do not have a confirmed pregnancy within the uterus.
-Pregnancy was conceived in a medically assisted way via a petri dish (in vitro fertilization)
-Uncertain if pregnant but patient has not had of a period for > 4 weeks before current symptoms started
-Patients who have unstable vital signs (dangerously low blood pressure, rapid heart rate) with sudden abdominal pain unexplained by other diagnosis.
-May also have no symptoms at all.
I have been diagnosed with an Ectopic Pregnancy. What is the treatment?
If you are diagnosed with an ectopic pregnancy, it can be a very scary. Your gynecologist will discuss many different options with you, some of which we will review here.
Your doctor will likely measure a hormone called beta human chorionic gonadotropin (B-hCG) in order to track the ectopic pregnancy. An ultrasound will also be performed in order to try to determine the location of the ectopic pregnancy (like in the picture above). Your blood pressure and heart rate will be checked along with a physical exam. Based on each of these factors, medical or surgical treatment may be offered. Your doctor will help you to determine the best course of treatment for you.
Call the UCR Silver Oaks Office at 844-827-8000 to schedule an appointment with one of our Gynecologists.
Resources:
- Clayton HB, Schieve LA, Peterson HB, et al. Ectopic pregnancy risk with assisted reproductive technology procedures. Obstet Gynecol 2006; 107:595.
- Bouyer J, Coste J, Fernandez H, et al. Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Hum Reprod 2002; 17:3224.
- Alkatout I, Honemeyer U, Strauss A, et al. Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv 2013; 68:571.